Antepartum nursing is high-stakes monitoring: preterm labor, preeclampsia, PPROM, placenta previa, IUGR, gestational diabetes — patients who are admitted because their pregnancy is too high-risk to manage outpatient. Your brain sheet tracks the status of each monitored pregnancy, the NST result from this morning, whether magnesium sulfate is running and at what rate, and which patient is due for betamethasone dose two. Download the free printable PDF below, or track your antepartum assignment digitally in NurseBrain Synapse so your notes are organized from morning NST to evening shift handoff.
What is an antepartum brain sheet?
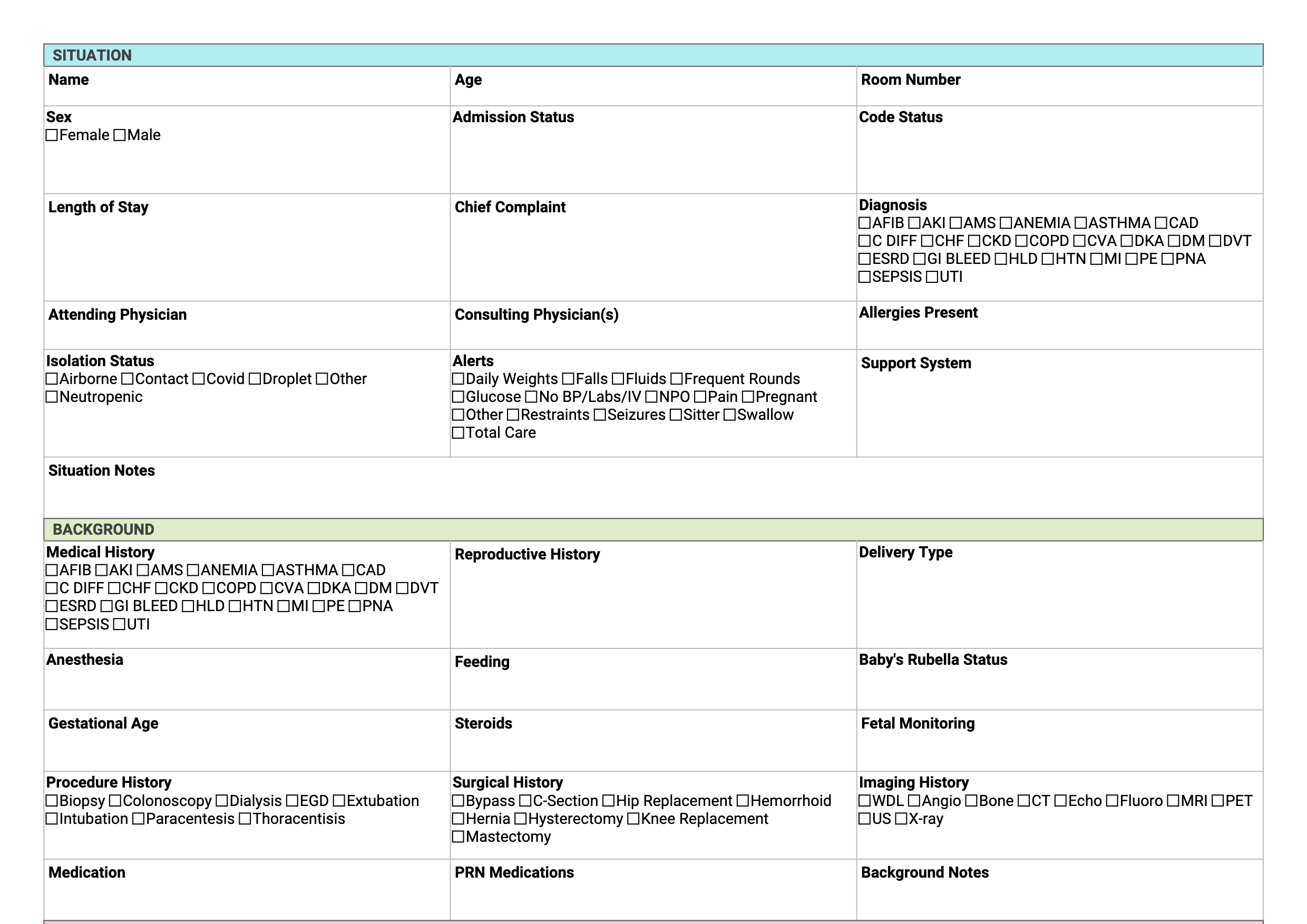
Antepartum units care for pregnant patients who need continuous or frequent monitoring but haven't delivered yet. The clinical complexity varies: one patient may be a straightforward preterm labor observation, another is a severe preeclamptic on magnesium with daily labs and strict I&O, and a third is a 28-weeker with PPROM counting fetal movements and getting fetal lung maturity steroids. The antepartum brain sheet tracks the unique monitoring parameters for each patient — fetal status, contraction frequency, medication drips, lab trends, and the gestational age clock that drives every clinical decision.
What to track on an antepartum brain sheet
Antepartum brain sheets typically cover: gestational age and estimated due date; admission diagnosis and primary concern; obstetric history (G/P, prior complications); current medications and infusions (magnesium, terbutaline, heparin, nifedipine, betamethasone doses and timing); fetal heart rate monitoring (NST results by date and time, BPP scores, Doppler studies); contraction frequency and character; cervical status (last check and result, if applicable); maternal vitals (BP trends especially for preeclampsia, reflexes, clonus if on magnesium); I&O (especially for preeclampsia or magnesium patients); laboratory values (CBC, BMP, coags, 24-hour urine protein, uric acid, LFTs); and planned delivery threshold or trigger criteria.
Antepartum brain sheet vs antepartum report sheet: same tool, complex patients
Antepartum nursing uses the same brain sheet concept as any other unit, but the content is more obstetric-specific: fetal movement counts, NST results, gestational age calculations, and diagnosis-specific monitoring like magnesium toxicity checks. The free PDF template organizes this in one place per patient. NurseBrain Synapse is the digital version — it keeps your monitoring log and medication timing organized so you don't have to reconstruct a week of antepartum notes when the patient finally delivers.
Antepartum Nurse FAQ
What does an antepartum nurse do?
An antepartum nurse monitors and cares for high-risk pregnant patients who require hospitalization before delivery. This includes continuous or scheduled fetal heart rate monitoring, NST and BPP interpretation, managing preeclampsia patients on magnesium sulfate, administering betamethasone for fetal lung maturity, monitoring preterm labor patients on tocolysis, doing daily assessments on patients with PPROM, IUGR, placenta previa, or gestational diabetes, and educating patients on fetal movement counting and warning signs for their specific condition.
How many patients does an antepartum nurse take?
Antepartum ratios vary by acuity. A nurse managing a severe preeclamptic on magnesium with strict I&O is often 1:1 or 1:2. Stable antepartum patients on monitoring without active treatment may have ratios of 1:3 or 1:4. The staffing depends heavily on the number of actively managed patients (Pitocin, magnesium, continuous monitoring) versus observation patients.
What is a non-stress test and what should I document?
A non-stress test (NST) uses electronic fetal monitoring to evaluate fetal wellbeing without a contraction stress. A reactive NST shows two or more accelerations of 15 bpm above baseline lasting at least 15 seconds within a 20-minute window. Document the start and end time, whether the NST was reactive or non-reassuring, fetal heart rate baseline and variability, any decelerations, whether vibroacoustic stimulation was used, and the provider notification and response if the result was non-reactive.
What are signs of magnesium toxicity I should monitor?
Magnesium sulfate toxicity progresses in stages. Early signs: flushing, nausea, headache, loss of patellar reflexes (usually first to go — check reflexes every hour). Respiratory depression occurs at higher serum levels; respiratory arrest at toxic levels. Monitor patellar reflexes, respiratory rate (keep >12), urine output (keep >30 mL/hr), and level of consciousness every 1–2 hours. Have calcium gluconate at the bedside as the antidote.
Can I use a digital antepartum brain sheet?
Yes. NurseBrain Synapse works on your phone or tablet. You can log NST results, magnesium rates, betamethasone timing, BP trends, and daily lab values digitally so your antepartum monitoring record stays organized across a long inpatient stay. Available on iOS and Android.