Why are care plans necessary?
The short answer is: “Proper Preparation Prevents Poor Performance!” The formal answer is: Care plans are an important tool used to plan and provide personalized care to your patients through the implementation of the Nursing Process (ADPIE). They help you be more deliberate in the nursing care you provide.
Follow along with our Free Care Plan Builder!
Our patient is a 54 y/o female with a primary diagnosis of Congestive Heart Failure (CHF). She presented to the emergency room complaining of shortness of breath on exertion.
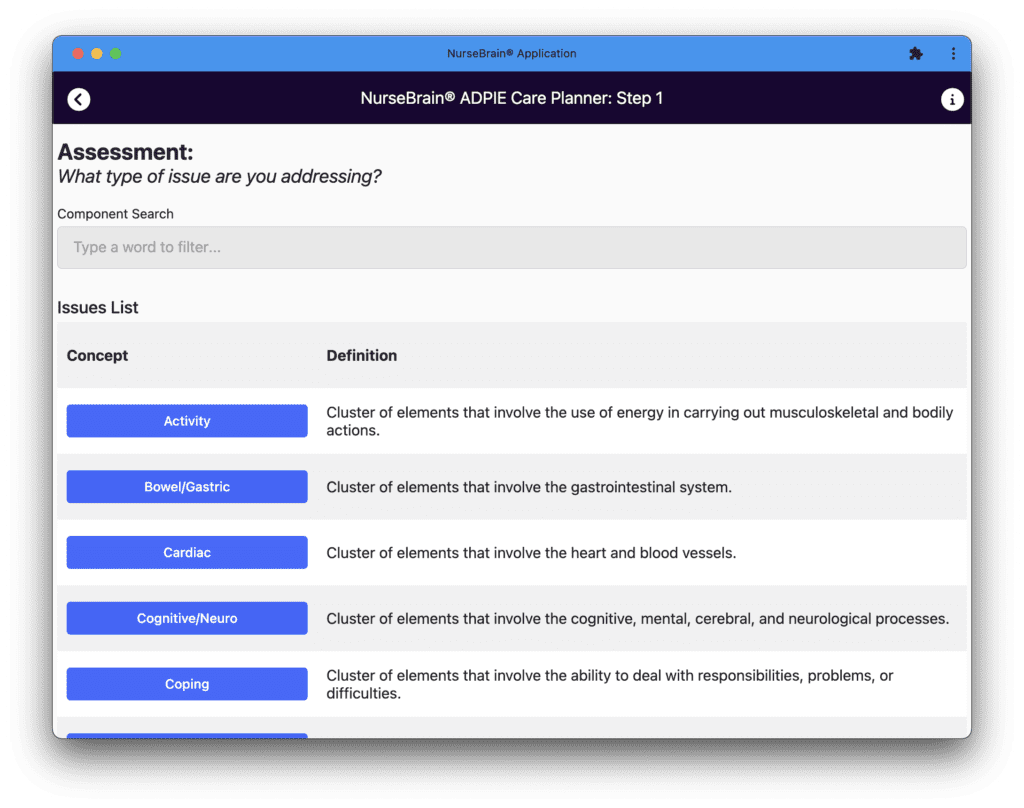
- Assessment
- In the assessment, we identify the issue we are addressing. In this case, we are concerned by the patient’s cardiac condition due to their CHF diagnosis. So we go ahead and select the “Cardiac” button.
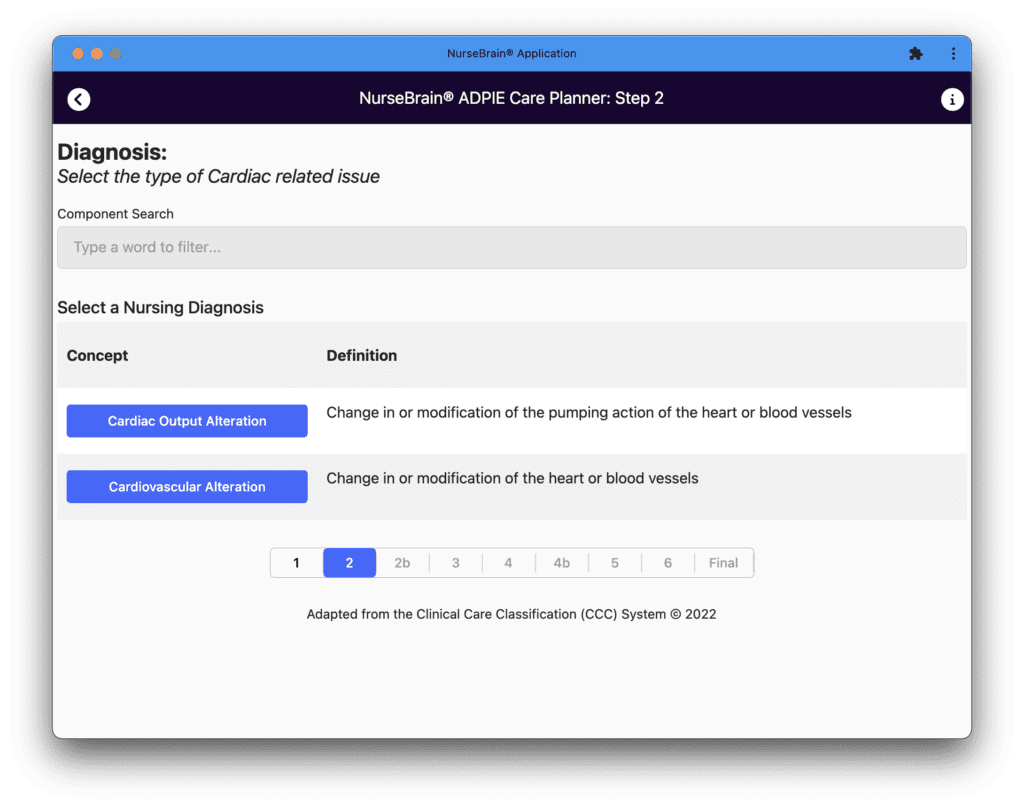
- Diagnosis
- For the diagnosis, we refine a bit more the type of cardiac issue we are addressing. We know that for patients suffering from congestive heart failure, cardiac output is often affected. We therefore proceed by selecting the “Cardiac Output Alteration” button.
-
-
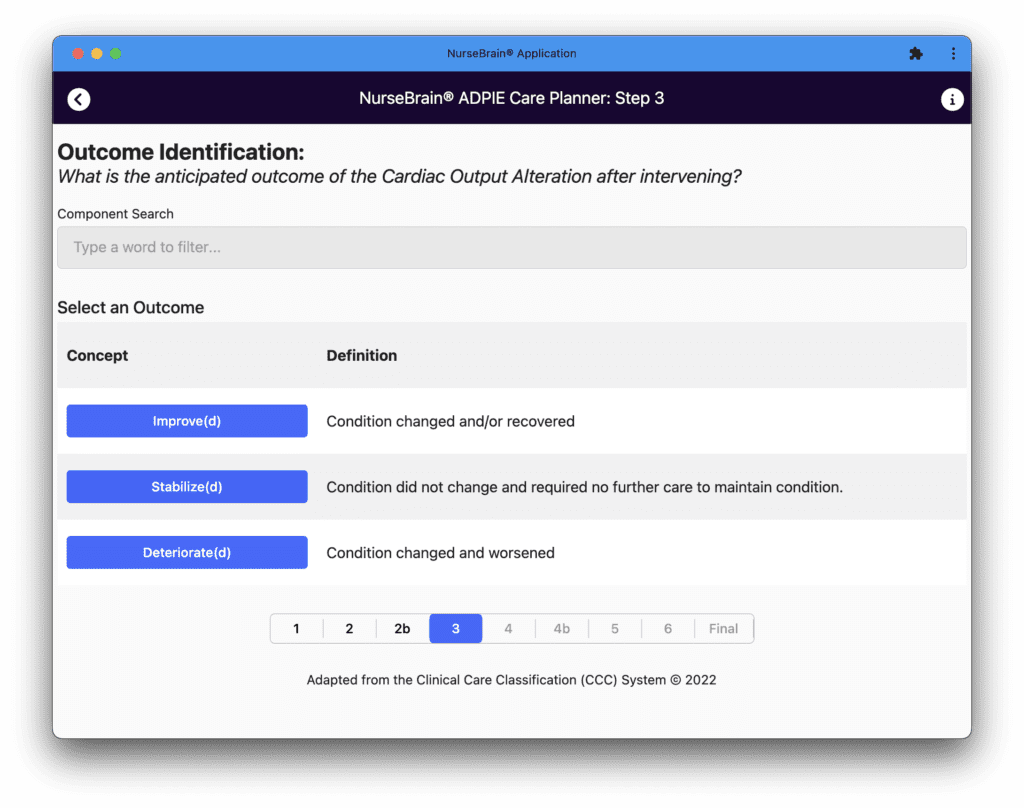
- Outcome Identification
- To complete the nursing diagnosis, we identify the expected outcome of the nursing diagnosis once we have implemented the proper interventions. We want the patient’s condition to improve so they can resume their usual activities of daily living without distress. So we select the “Improve” button to continue.
- Outcome Identification
-
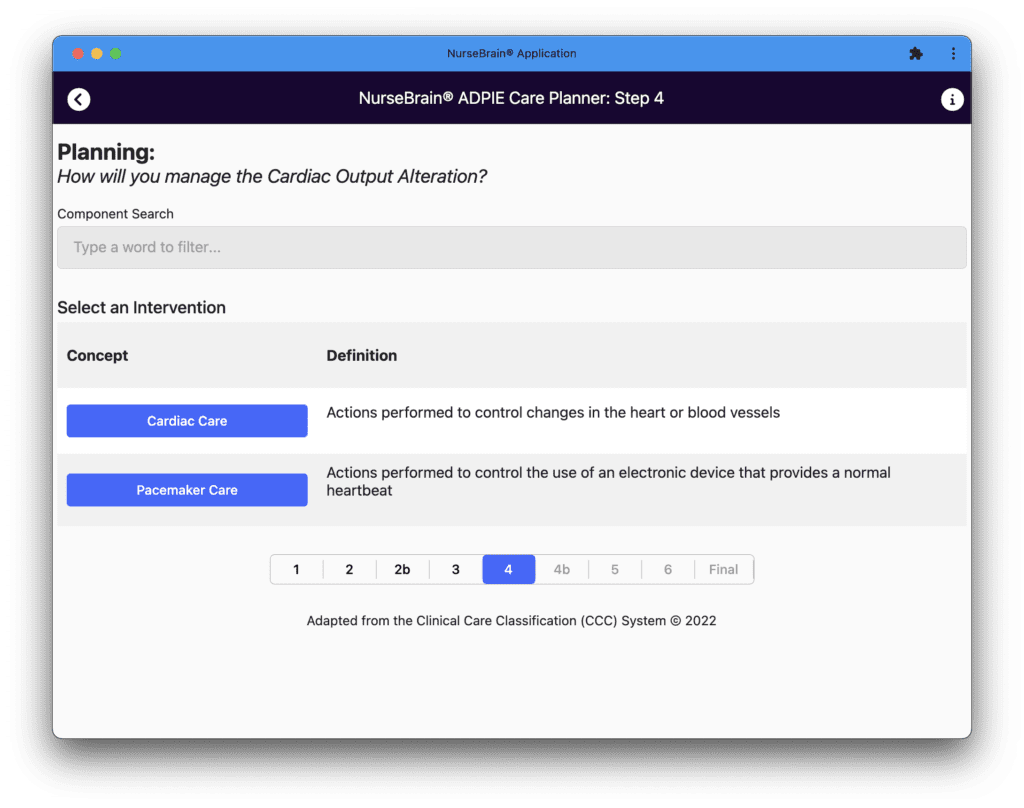
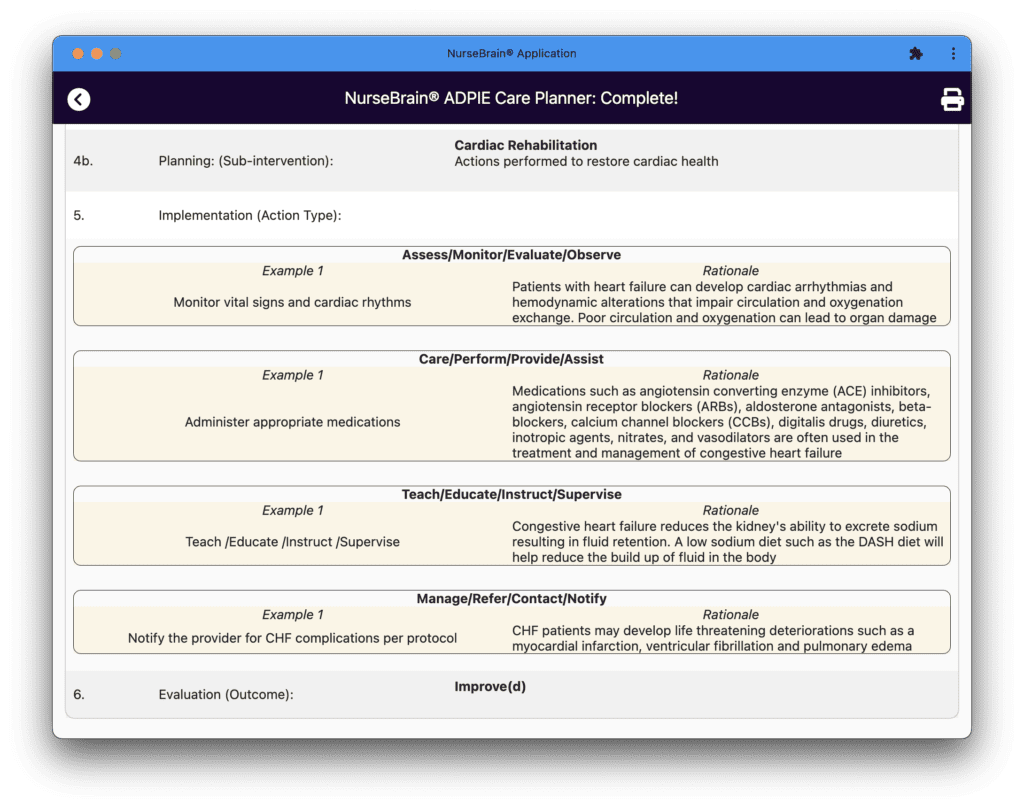
- Planning (Intervention / Sub-Intervention)
- After identifying an expected outcome, we have to make a plan on how to reach our goal of improving the patient’s cardiac out alteration. Our plan will comprise of interventions that provide Cardiac Care within our scope of practice. Let’s proceed by selecting the “Cardiac Care” button followed by “Cardiac Rehabilitation.”
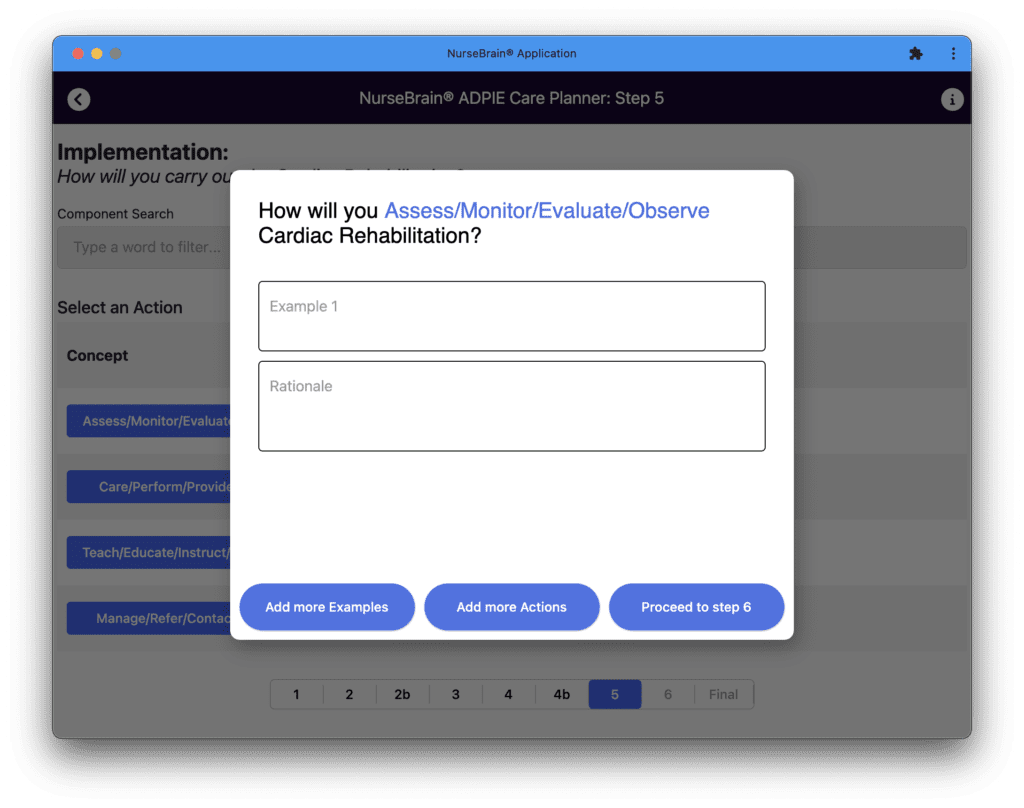
- Implementation
- After assessing, diagnosing and planning, we now get to implement our interventions! We will do so by tapping the appropriate buttons and entering examples of actions we are/will take while providing the respective rationales.
- Congestive Heart Failure Actions & Rationales
- Monitor /Assess /Evaluation /Observe
- Monitor vital signs and cardiac rhythms
- Patients with heart failure can develop cardiac arrhythmias and hemodynamic alterations that impair circulation and oxygenation exchange. Poor circulation and poor oxygenation can lead to organ damage
- Monitor vital signs and cardiac rhythms
- Perform /Direct Care /Provide /Assist
- Administer appropriate medications
- Medications such as angiotensin converting enzyme (ACE) inhibitors, angiotensin receptor blockers (ARBs), aldosterone antagonists, beta-blockers, calcium channel blockers (CCBs), digitalis drugs, diuretics, inotropic agents, nitrates, and vasodilators are often used in the treatment and management of congestive heart failure
- Administer appropriate medications
- Teach /Educate /Instruct /Supervise
- Teach patient importance of a low sodium diet
- Congestive heart failure reduces the kidney’s ability to excrete sodium resulting in fluid retention. A low sodium diet such as the DASH diet will help reduce the build up of fluid in the body and help minimize complications
- Teach patient importance of a low sodium diet
- Manage /Refer /Contact /Notify
- Notify the provider for CHF complications per protocol
- CHF patients may develop life threatening deteriorations such as myocardial infarctions, ventricular fibrillation and pulmonary edema
- Notify the provider for CHF complications per protocol
- Monitor /Assess /Evaluation /Observe
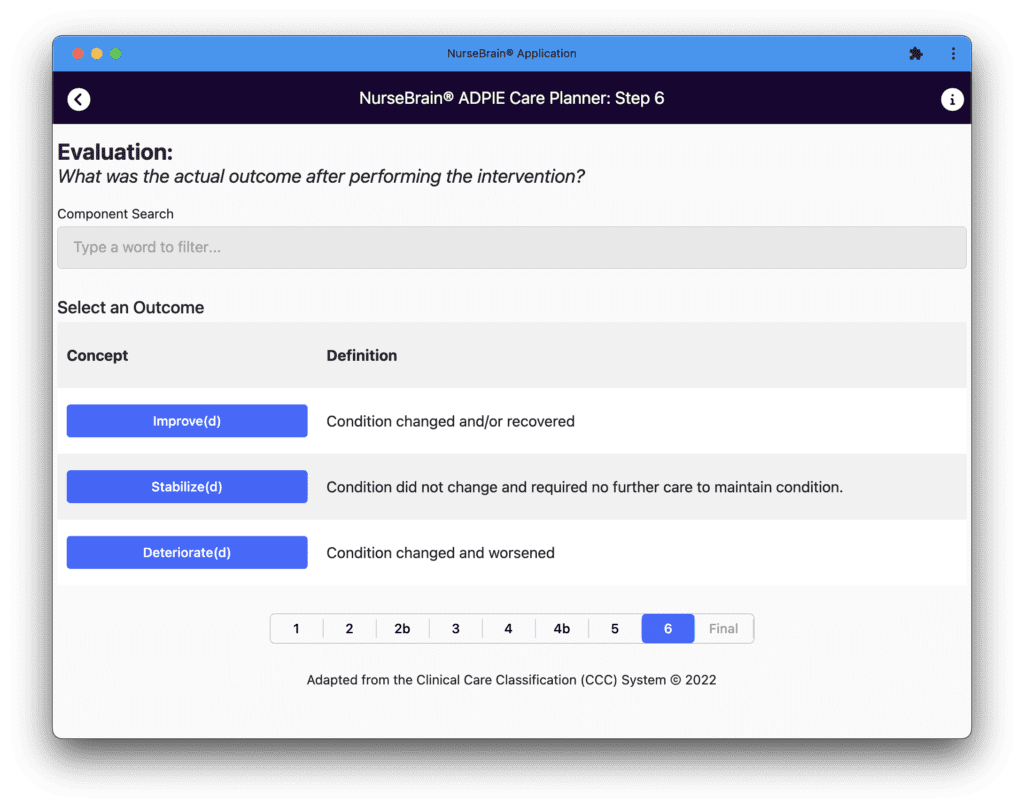
- Evaluation
- In this last step of the Nursing Process, we evaluate our plan of care to see if it worked or needs some alterations. Fortunately for our patient, we made the appropriate diagnosis, created a personalized plan of care and intervened using evidence based actions. Our patient’s condition improved and she is now ready to be discharged pending final clearance form the provider. We will conclude by selecting the “Improved” button.
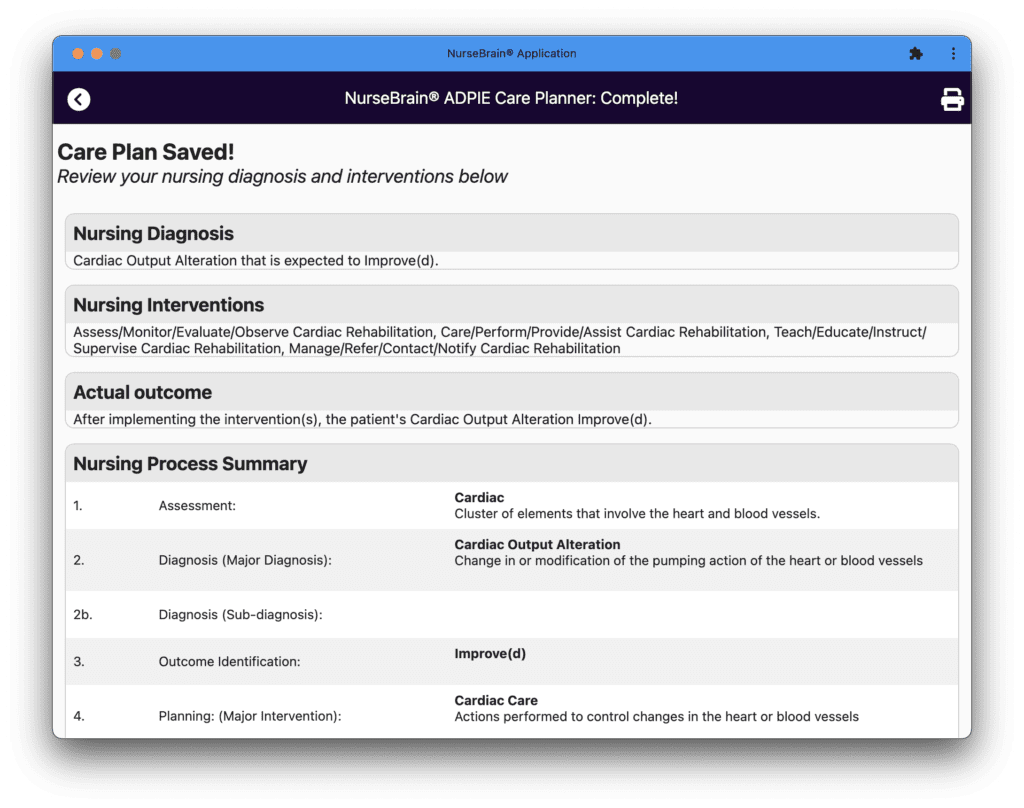
Summary
The Clinical Care Classification System is an evidence based tool for creating care plans based on the Nursing Process: Assess, Diagnose, Plan, Implement & Evaluate. Using the Nursing Process helps nurses be more deliberate in providing comprehensive care to their patients. You can use the NurseBrain Care Planner tool for free at the NurseBrain website. Download this sample patient and care plan.
Related Free Resources
Put it into practice: build a free brain sheet at nursebrain.com/sheets, or work through a fully written example with our free nursing care plans (25+ conditions with pathophysiology, nursing diagnoses, labs, meds, and red flags).